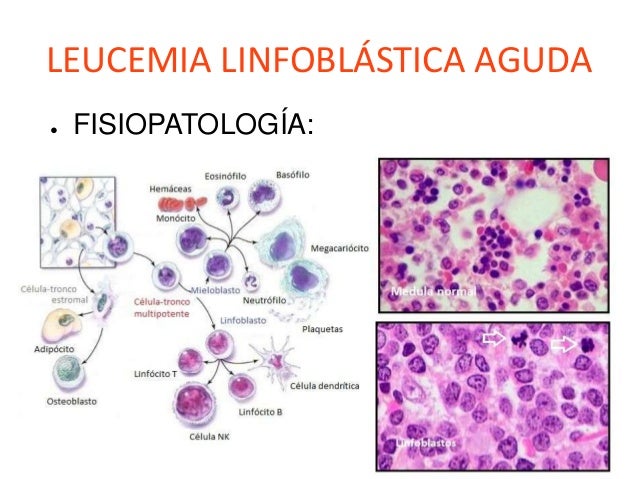
LEUKEMIA
General features
Leukemia is a cancer of the blood cells. Most blood cells are formed in the bone marrow. In the case of leukemia, immature blood cells become cancerous. These cells do not work as they should and congested to healthy blood cells in the bone marrow.
The different types of leukemia depends on the type of blood cell that becomes cancerous. For example, lymphoblastic leukemia is a cancer of the lymphoblasts (white blood cells that fight infection). White blood cells are the most common type of blood cell that becomes cancerous. However, red blood cells (cells that carry oxygen from the lungs to the body) and platelets (blood clotting cells) may also be converted into cancer.
Leukemia is more common in adults over 55 years, but is also the most common cancer in children under 15 years.
Leukemia can be acute or chronic. Acute leukemia is a fast-growing cancer usually gets worse quickly. Chronic leukemia is a slow-growing cancer that slowly gets worse over time. The treatment and prognosis of leukemia depends on the type of blood cell affected and the leukemia is acute or chronic.

personal opinion
I chose this topic because it is important that we identify the characteristics of this enfemermedad, which can be treated and have a treat for people to have a life of health, no matter what social status you have, the most important thing is that we knowledge and help prevent leukemia, I like to talk about it because they are simple topics to speak, therefore I am presenting clear and summarized information for the reader to understand and analize the information,
bibliographya
Gerardo Garcia Peralta . (2010). generalidades de la leucemia . 5/10/2015, de leucemia Sitio web: http://www.cancer.gov/espanol/tipos/leucemia
Etiology of leukemia
The indiscriminate use of X-rays and some drugs, especially in children and pregnant women. Severe bad nutrition, excessive consumption of refined carbohydrates (especially in children), excessive water fluoridation or salt, thyroid malfunction, vitamin D deficiency, iron, vitamin B12 and folic acid, chronic viral infections, hereditary propensity.
Symptoms:
paleness
purple bleeding fever
increased joint pain vulumen
abdominal pain
Leukemia almost always occurs as a mixture of several basic syndromes: anemic (the most common), fever, bleeding, tumor and pain (bone). In this case series was 66% pale, half of them also had a fever and was bleeding 1/3; in 18 cases it was associated with bone pain and 10 to volume increases. However there were 14 patients whose only symptom was pale, being in them very important to evaluate physical examination and blood count. Fever is a common symptom and evidence in this review that the analysis of blood count is very important because 60 cases of febrile neutropenia were 42, 17 and one blasts presence of anemia. In 4 of these 60 children the fever was the only symptom and all the blood count showed neutropenia.
personal opinion:
It is important to know, which causes this disease and avoid bad avitos, and must identify the symptoms, to prevent leukemia, thanks to early detection can be achieved by a treatment to help eliminate the disease. today there espesificos treatments which allows the disease does not progress and the sick person can get healthy

bibliography
Myriam Campbell B. (6/1999). leucemia etiologia y síntomas . 7/10/2015, de scielo Sitio web: http://www.scielo.cl/scielo.php?pid=S0370-41061999000400004&script=sci_arttext
8/10/2015
The blood components
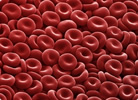
Red blood cells
Also called erythrocytes. They are most numerous blood cells. They are responsible for transporting oxygen from the lungs to other tissues. The protein found inside and linking oxygen is called hemoglobin. Hemoglobin is red and gives this color to blood.
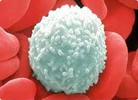
White Blood Cells
Also they called leukocytes. They concerned with defending the body against attack by bacteria, viruses, parasites and fungi.
Platelets or thrombocytes
Cell fragments are involved in protecting the wall of blood vessels, forming a "platelet plug" to prevent bleeding at the site of injury and produce various substances that help the healing of wounds.

plasma
It is the liquid part of the blood and is very rich in proteins, among which stand out as the most important: albumin, coagulation factors and immunoglobulins
personal opinion
Today they speak of blood components, because during the course of lecucemia to take, we'll be talking a lot about these Temino, and so will be much easier to understand the subject of the talk, mensiono leucositos, red blood cells, platelets and plasma, likewise put its function where the importance of this is shown, I hope you like this articuilo which is summarized but the information is understandable and clear.
bibliographia
Fundació Banc de Sang . (2012). que es la sangre . 8/10/2015, de dona sangre Sitio web: http://www.donasang.org/que-es-la-sang/es_els-components.html
12 de october,2015
Leukemia in children
The symptoms of leukemia are often caused by problems in the child's bone marrow, where leukemia begins. As the leukemia cells accumulate in the bone, they can displace cells producing normal blood cells. As a result, a child may not have enough red blood cells, white blood cells or platelets. These shortages show up on blood tests, but they can also cause symptoms. Leukemic cells may also invade other body areas, which can also cause symptoms.
Symptoms caused by low red blood cell counts (anemia) Red blood cells carry oxygen to all body cells. A decrease in red blood cells may cause:
Tiredness (fatigue)
Soft spot
Feeling cold
Dizziness or lightheadedness
Headaches
Difficulty breathing
Pale skin
Symptoms caused by low white blood cells:
Infections can occur due to a shortage of normal white blood cells. Children with leukemia may get infections that can not seem to go away or get an infection after another. Although people with leukemia can often have a high white blood cell count because they have many leukemia cells, these cells do not protect against infection the way they do normal white blood cells.
Fever is often the main sign of infection. However, some children may have a fever without infection.
Symptoms caused by low platelet counts: platelets in the blood normally help stop bleeding. A reduced number of platelets can cause:
Tendency to easy bruising and bleeding
Frequent or severe nosebleeds
Bleeding gums
Bone pain or joint: the pain is caused by the accumulation of leukemia cells near the surface of the bone or inside the joint.
Swelling of the abdomen: the leukemia cells may collect in the liver and spleen, causing them to enlarge. This may be noticed as a fullness or swelling of the abdomen. The lower ribs usually cover these organs, but when they are enlarged the doctor often palpable.
Loss of appetite and weight: If the spleen and / or liver is enlarged too, can pressure other organs such as the stomach. This can cause the child to feel full after eating only a small amount of food, resulting in loss of appetite and weight loss over time.
Swollen lymph nodes: Some leukemias spread to the lymph nodes. You can see and feel enlarged nodes as lumps under the skin in certain areas of the body (such as the sides of the neck, underarm areas, above the collarbone or groin). Swollen lymph nodes found inside the chest or abdomen, but this can only be observed by imaging studies such as CT or MRI may also occur.
In infants and children, lymph nodes often enlarge when fighting off an infection. An enlarged lymph node in a child is much more often a sign of infection of leukemia, but a physician should make a thorough review and monitoring.
Cough or difficulty breathing: some types of leukemia may affect the structures in the center of the chest, such as lymph nodes or thymus (a small organ located in front of the trachea, breathing conduit leading to the kidneys). Enlarged thymus glands or lymph nodes in the chest can press the trachea, causing coughing or trouble breathing. In some cases where the white blood cell count is very high, the leukemia cells can build up in the small blood vessels of the lungs, which can also cause difficulty breathing.
Swelling of the face and arms: the superior vena cava (superior vena cava SVC), a large vein that carries blood from the head and arms back to the heart, passes near the thymus. An enlarged thymus can press the SVC causing blood to "back off" in the veins. This is called SVC syndrome, and can cause swelling of the face, neck, arms and upper chest (sometimes with a bluish-red coloration of the skin). It can also cause headaches, dizziness and, if it affects the brain, a change in consciousness. This syndrome can be life threatening and requires immediate treatment.
Headaches, seizures and vomiting: a few children have leukemia that has already spread to the brain and spinal cord when they are diagnosed. This can lead to symptoms such as headache, difficulty concentrating, weakness, seizures, vomiting, balance problems and blurred vision.
Rashes, gum problems: in children with acute myeloid leukemia (AML), the leukemia cells may spread to the gums, causing inflammation, pain and bleeding. If they spread to the skin, it can give rise to small dark points that may seem a common eruption. An accumulation of AML cells under the skin or other body parts or chloroma called granulocytic sarcoma.
Extreme fatigue, weakness: a rare, but very serious consequence of AML is extreme tiredness, weakness and difficulty speaking. This can occur when a large number of leukemia cells causes blood to become too thick and is made slower flow through the small blood vessels of the brain.
Again, it is likely that most of the symptoms listed above to a different ailment leukemia due. Still, it is important that a doctor examine him to determine and treat the cause of symptoms, if necessary.

personal opinion
now tell you about the symptoms that leukemia in children, symptoms previously mentions them in adults, ho me focus on the symptoms presented by children, parents or family as much as we must take them into account. to help a atiempo taratamiento and prevent disease progression as children wear a life ahead of therefore must have this knowledge and prevent
bibliography
Marta Carrillo Torres . (2010). leucemia en niños . 12 de octubre 2015, de leucemia generalidades Sitio web: http://www.cancer.org/espanol/cancer/leucemiaenninos/guiadetallada/leucemia-en-ninos-early-signs-and-symptoms
14 /10/2015
acute lymphoblastic leukemia
Acute lymphoblastic leukemia (ALL) is the most common cancer in childhood. The
immunophenotype of leukemic cells is one of the factors that set risk of relapse. The choice of
antibodies for diagnostic panel immune ALL may vary between institutions. Not all cases of ALL
express antigens for a single lineage as many cases have been reported where cells express the
characteristics of more than one hematopoietic lineage. According to different criteria there
are definitions of ALL with aberrant expression of antigens, lineage infidelity, mixed lineage,
and biphenotypic leukemias (BAL). The European Group of Immunological Classification of Leukemia
(EGIL) created a points-based system to distinguish BAL of those with aberrant expression.
It is based on the number and degree of specificity markers (lymphoid and myeloid cells)
expressed in leukemic cells.
Methods: We conducted a retrospective study at Hospital Infantil de México; we reviewed the
clinical records of 113 patients diagnosed with ALL in a period from 2008 to 2010. EGIL group
classification was used to determine if ALL had the criteria to BAL.
Results: One hundred thirteen clinical records were analyzed, 29 patients were identified as
standard-risk and 84 as high risk patients. In 32 cases it was found BAL by EGIL criteria, this corresponded
to 28.3% of the total sample. The group which had the highest number of BAL was the
group of high risk of relapse (25 patients with high-risk against 7 patients with standard
risk group).
Conclusions: This study is an attempt to classify systematically acute leukemia, however remains
to know if this diagnosis impact on outcome
personal opinion
today I wanted to talk about the lymphoblastic leukemia in methods and results, this is a very similar to previous themes feature, this is more common in children, and I will explain that cosnsite the method that results from it is carried out and, note that this is a type of leukemia, and affects different symptoms and characteristics are very different from other types of leukemia
bibliography :Dr. Jorge Martínez Cedillo. (3, MAYO - JUNIO 2013). leucemia linfoblastica aguda . 14/10/2015, de sociedad nacional de oncologia Sitio web: file:///C:/Documents%20and%20Settings/Administrador/Escritorio/oncologia.pdf
16 /10/2015
DIAGNOSIS
To diagnose acute leukemia several tests are needed to confirm this:
CBC: finding of more than 20% blasts in peripheral blood, anemia, thrombocytopenia, leukocytosis -> Morphology of cells describing the characteristics of the nucleus and cytoplasm on the basis of normal hematopoiesis
Bone marrow tests: Myelogram and Core Biopsy
Immunophenotype determines the lineage of neoplastic cells (myeloblast, lymphoblast, lymphocyte, etc.) through surface markers which are detected by flow cytometry
Cytogenetics and Molecular Biology: searches for possible genetic and cytogenetic alterations associated to the prognosis of the disease that the patient
Cytochemical staining (only occasions)
What Is a Bone Marrow Biopsy?
Why Is a Bone Marrow Biopsy Done?

Personal opinion, today diagnostic Talk to them to know that the paciete has leukemia, but I focus on talk of expiration of the bone marrow, this is a sterile technique in which liquid is removed from the bone marrow and sent to inspect, a tenber probability of disease
BIBLIOGRAPHY
Francisco Rivera . (2011). leucemia y diagnostico . 16/10/2015, de LEUKEMIA TIME Sitio web: http://www.healthline.com/health/bone-marrow-biopsy#Overview1
https://www.youtube.com/watch?v=NkdsLHBCreI
Monday October 21 2015
How is childhood leukemia classified
The type of leukemia a child has played an important role in both treatment options and prognosis of the child. Determining the type (acute lymphocytic, acute myeloid, etc.) and subtype of leukemia ago analyzing samples of blood, bone marrow, and sometimes lymph nodes or cerebrospinal fluid (as described in "How is it diagnosed the childhood leukemia? ").
For most types of cancer, determining the stage (extent) of cancer it is important. The stage is based on tumor size and how far the cancer has spread. However, leukemia not staged as most other cancers. Leukemia begins in the bone marrow and spreads quickly into the blood. Therefore, from the beginning the leukemia cells are already scattered throughout the body.
Still, it is important to know whether the leukemia cells have already begun to accumulate in other organs such as the liver, spleen, lymph nodes, testes or central nervous system (brain and spinal cord). For example, if a large number of leukemia cells has spread to the central nervous system will be detected in samples of cerebrospinal fluid. The treatment should be more intense to destroy these leukemic cells. For this reason, a lumbar puncture is part of early diagnostic tests.
Acute lymphocytic leukemia (lymphoblastic)
Acute lymphocytic leukemia (ALL) is a fast-growing cancer of lymphocytes producing cells, called lymphoblasts.
Classification based on appearance (morphology) of leukemic cells
In the past, doctors used the French-American-British (FAB) classification to divide ALL into three major groups (L1, L2 or L3) based on how the cells look under the microscope. Some doctors may even refer to these categories. However, newer lab tests now allow doctors to classify ALL based on more than just how the cells look under the microscope.
Classification based on immunophenotype
New types of laboratory tests can help determine the subtype of ALL and the patient's prognosis. These tests help divide ALL into groups based on the immunophenotype of leukemia:
The type of lymphocyte (B cell or T cell) the leukemia cells come.
How mature are these leukemia cells.
B cell ALL: In about 80% to 85% of children with ALL, leukemia begins on B cells Several subtypes of B cells:
ALL of early precursor B cells (also called pro-B ALL)
Common ALL
Pre-B ALL
ALL mature B cells (also called Burkitt leukemia) This type is rare, accounting for only about 2% to 3% of childhood ALL. It is essentially the same as Burkitt's lymphoma and is different from most leukemias. It is addressed in detail in our document NHL children.
T-cell ALL: approximately 15-20% of children with ALL have a T-cell ALL This type of leukemia affects boys more than girls, and usually affects children older than cell ALL B. This type of leukemia often causes an enlarged thymus (a small organ located in front of the windpipe), which can sometimes cause breathing problems. It can also spread to the cerebrospinal fluid (the fluid that surrounds the brain and spinal cord) in the early stages of the disease.
In addition to the subtype of ALL, other factors are important for determining the prognosis (outlook). These factors are described in the "Prognostic factors in childhood leukemia" section.
Acute myeloid leukemia (AML)
Acute myeloid leukemia (AML) is usually a fast-growing cancer of one of the following types of early cells (immature) bone marrow:
Myeloblasts: these cells normally form white blood cells called granulocytes (neutrophils, eosinophils and basophils).
Monoblasts: These cells normally become white blood cells called monocytes and macrophages.
Erythroblasts: These cells become red blood cells as they mature.
Megakaryoblasts: these cells normally become megakaryocytes, platelet-producing cells.
They have been using two systems to classify AML into subtypes: the French-American-British (FAB) classification and the most recent classification of the World Health Organization.
French-American-British (FAB) classification of acute myeloid leukemia (AML)
The former FAB system divides AML into subtypes, depending on the type of cell from which leukemia and maturity of the cells originated. In this system, the subtypes of AML are classified primarily by their morphology (how they look under a microscope). There are eight subtypes of AML: M0 to M7 (M refers to myeloid).
M0: undifferentiated acute myeloid leukemia
M1: acute myeloblastic leukemia with minimal maturation
M2: acute myeloblastic leukemia with maturation (the most common subtype of AML in children)
M3: acute promyelocytic leukemia (APL)
M4: acute myelomonocytic leukemia (most common in children under two years old)
M5: acute monocytic leukemia (most common in children under two years old)
M6: Acute erythroid leukemia
M7: Acute Leukemia megakaryoblastic
Subtypes M0 to M5 all start in immature white blood cells. M6 AML begins in immature red blood cells, while M7 AML begins in immature cells that produce platelets.
AML classification of the World Health Organization (WHO)
The FAB classification system is still commonly used to group AML into subtypes. However, it does not take into account many other factors that are known to affect prognosis, such as chromosomal changes in the leukemia cells. The latest system of the World Health Organization (WHO) includes some of these factors to help better classify the AML based on a person's outlook.
The WHO system divides AML into several groups:
AML with certain genetic abnormalities
AML with a translocation between chromosomes 8 and 21
AML with a translocation or inversion on chromosome 16
AML with a translocation between chromosomes 9 and 11
APL (M3) with a translocation between chromosomes 15 and 17
AML with a translocation between chromosomes 6 and 9
AML with a translocation or inversion on chromosome 3
AML (megakaryoblastic) a translocation between chromosomes 1 and 22
AML with myelodysplasia-related changes
AML related to previous chemotherapy or radiation
AML not otherwise specified (this includes cases of AML not corresponding to one of the above groups, and is similar to the FAB classification.)
AML with minimal maturation (M1)
AML with maturation (M2)
AML with maturation (M2)
Acute myelomonocytic leukemia (M4)
Acute monocytic leukemia (M5)
Acute erythroid leukemia (M6)
Acute megakaryoblastic leukemia (M7)
Acute basophilic leukemia
Panmyelosis with acute Fibrosis
Myeloid sarcoma (also known as chloroma or granulocytic sarcoma)
Myeloid proliferations related to Down syndrome
Biphenotypic acute undifferentiated leukemias (lymphocytic leukemias having features and myeloid). These are also known as mixed phenotype leukemia or mixed-lineage leukemia. In children, these leukemias are generally treated like ALL and usually respond to treatment like ALL.
Chronic myeloid leukemia (CML)
Chronic myeloid leukemia (CML) is usually a slower early myeloid cells (immature) bone marrow cancer growth. CML is rare in children, but can occur in them.
The course of CML is divided into three phases, based primarily on the number of immature white blood cells (myeloblast ["blasts"]), observed in the blood or bone marrow. Different groups of experts have suggested slightly different boundaries to define the stages, but then a common system (defined by the World Health Organization) is described.
If the leukemia does not heal with treatment, it can progress to more advanced stages with the passage of time.
Chronic Phase
This is the earliest phase in which patients usually have less than 10% blasts in samples of blood or bone marrow. These children usually have fairly mild symptoms (if any present), and leukemia usually responds well to conventional treatments. Most patients are in the chronic phase when they are diagnosed.
Accelerated phase
It is considered that patients are in an accelerated phase if samples of blood or bone marrow have more than 10% but less than 20% blasts, or if the levels of certain blood cells are too high or too low.
Children whose CML is in accelerated phase may have symptoms such as fever, night sweats, loss of appetite and weight loss. The accelerated phase CML may not respond as well to treatment as CML in chronic phase.
Blastic phase (also called acute phase or blast crisis)
At this stage, samples of blood and / or bone marrow are more than 20% blasts. Blast cells often spread from bone marrow to other tissues and organs. These children often have fever, poor appetite and weight loss. At this point the CML behaves like an aggressive acute leukemia (AML or, less often, ALL).
bibliografhy
Mirian Cacis . ( 05/12/2015). Cómo se clasifica la leucemia en niños. 19/10/2015, de leucemia en niños Sitio web: http://www.cancer.org/espanol/cancer/leucemiaenninos/guiadetallada/leucemia-en-ninos-early-how-classifiedWednesday October 21, 2015
acute myeloid leukemia in adults
IMPORTANT POINTS
Acute myeloid leukemia (AML) in adults is a type of cancer in which the bone marrow produces abnormally, myeloblasts (a type of white blood cell), red blood cells or platelets.
Leukemia can affect red blood cells, white blood cells and platelets.
Different subtypes of acute myeloid leukemia.
Smoking, prior treatment with chemotherapy and radiation exposure may influence the risk of developing adult AML.
Signs and symptoms of acute myeloid leukemia in adults include fever, fatigue, easy bruising or bleeding.
To detect (find) and diagnose acute myeloid leukemia in adults, testing is used to examine the blood and bone marrow.
Certain factors affect prognosis (chance of recovery) and treatment options.
Acute myeloid leukemia (AML) in adults is a type of cancer in which the bone marrow produces abnormally, myeloblasts (a type of white blood cell), red blood cells or platelets.
Acute myeloid leukemia (AML) in adults is a cancer of the blood and bone marrow. This type of cancer usually gets worse quickly if treatment is not administered. It is the most common type of acute leukemia in adults. AML is known also called acute myelogenous leukemia, acute myelogenous leukemia, acute granulocytic leukemia and acute non-lymphocytic leukemia.
AMPLIARAnatomía bone; in the illustration, cancellous bone, red marrow and yellow marrow it is shown. In a transverse section of bone, compact bone and blood vessels in the bone marrow is. Red blood cells, white blood cells, platelets and blood stem cells are also shown.
Bone anatomy. The bone is composed of compact bone, cancellous bone and marrow. Compact bone forms the outer layer of the bone. Cancellous bone is, above all, to the ends of bones and contains red marrow. The bone marrow is in the center of most bones and has many blood vessels. There are two types of bone marrow: red and yellow. Blood red marrow contains stem cells that can be converted into red cells, white cells or platelets. Yellow marrow is composed, for the most part, of fat.
Leukemia can affect red blood cells, white blood cells and platelets.
Bone marrow typically blood stem cells (immature cells) that eventually develop into mature blood cells. A blood stem cell may become a myeloid stem cell or a lymphoid stem cell. A lymphoid stem cell develops into a white blood cell.
A myeloid stem cell becomes one of three types of mature blood cells:
Red blood cells that carry oxygen and other materials to all tissues of the body.
White blood cells that fight infection and disease.
Platelets that form blood clots to stop bleeding.

personal opinion :
today I speak briefly of myeloid leukemia in adults, the disease tells us that specifically affects adults, and it affects red blood cells, white blood cells and platelets, and the main symptoms are fatigue and emorragias this disease can be detected atiempo with a blood test, it is very important that when symptoms occur can seek medical and request a blood chemistry test is very important to prevent progress myeloid leukemia.
bibliogrphy : National Cancer Institute. (1 de octubre de 2015). leucemia mieloide . 21/10/2015, de instituto nacional de cancer Sitio web: http://www.cancer.gov/espanol/tipos/leucemia/paciente/tratamiento-lma-adultos-pdq
Friday October 23, 2015
detection and treatment of myeloid leukemia in adults
You can use the following tests and procedures:
Physical exam and history: An exam of the body to check general health and identify any signs of disease, such as lumps or anything else that seems unusual. Data on the patient's health habits, previous diseases and treatments applied in each case are also taken.
Complete blood count (CBC): A procedure in which a sample of blood is drawn and checked for the following:
The number of red cells, white cells and platelets.
The amount of hemoglobin (the protein that carries oxygen) in red blood cells.
The portion of the sample made up of red blood cells.
Peripheral blood smear: A procedure in which a blood sample is analyzed to check blastocysts, the number and types of white blood cells, platelet count and changes in the shape of blood cells.
Bone marrow aspiration and biopsy: The removal of bone marrow, blood and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow, blood, and bone under a microscope to check for signs of cancer.
ENLARGE


Personal opinion: today I want to talk about the diagnosis you can perform to esactamente detect leukemia, note that the symptoms do not see at first glance, this requires evidence; siertas, and thereby have serteros results, and there to take treatment required by the patient agreement
bibligraphy
National Cancer Institute. (1 de octubre de 2015). leucemia mieloide . 23/10/2015, de instituto nacional de cancer Sitio web: http://www.cancer.gov/espanol/tipos/leucemia/paciente/tratamiento-lma-adultos-pdq
Monday October 26, 2015
Chemotherapy for acute lymphocytic leukemia
Chemotherapy (chemo) is the use of drugs to treat cancer. Most often, these drugs are injected into a vein, into a muscle, under the skin or taken by mouth. The drugs travel through the bloodstream to reach cancer cells throughout the body. This makes chemotherapy useful for cancers such as leukemia that has spread throughout the body treatment. Most chemotherapies do not reach the area right around the brain and spinal cord. For this reason, it may be necessary to inject chemotherapy into the spinal fluid to kill cancer cells in that area. This is called intrathecal chemotherapy.
Typically the treatment is done in three phases:

Induction (or remission induction).
Consolidation (intensification)
Maintenance
The total treatment usually takes about two years, with the maintenance phase which requires more time. Treatment may be more or less intense, depending on the subtype of ALL and other prognostic factors.
The ALL may spread to the area around the brain and spinal cord. Sometimes, this has already happened when first made the diagnosis of ALL. This spread is discovered when the doctor makes a lumbar puncture and leukemic cells are seen by examining the fluid under a microscope. The treatment for this is discussed below.
Although no leukemia cells are found in the cerebrospinal fluid at diagnosis, you may have very few cells so that these tests might recognize or they could start subsequently grow on the surface of the brain and spinal cord. For this reason, an important part of treatment for ALL is the central nervous system prophylaxis, a treatment that aims to ensure that the leukemia does not spread to the area around the brain or spinal cord. This is also described in more detail below.
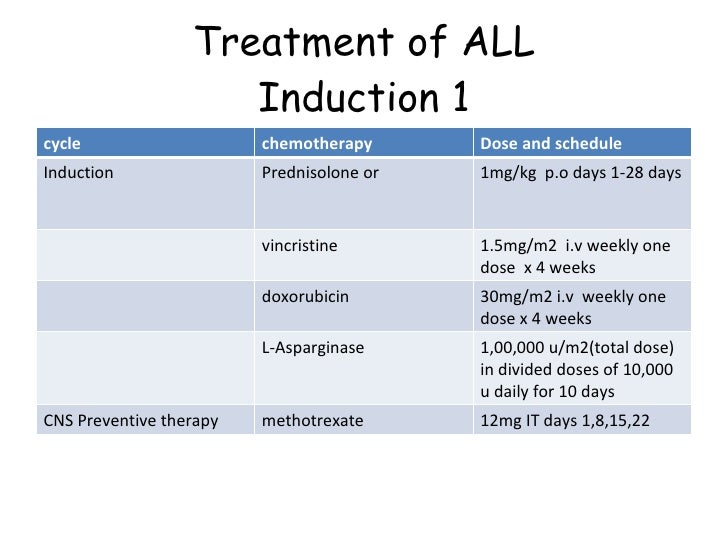
Induction
The goal of induction chemotherapy is a referral. This means that leukemia cells are no longer found in bone marrow samples, returning normal marrow cells and blood counts are normal. However, a referral is not necessarily a cure, because the leukemic cells could still be hiding somewhere in the body.
This is a phase of intensive chemotherapy usually lasts for a month or so. Maybe different combinations of chemotherapy drugs are used, but typically includes:
Vincristine
Dexamethasone or prednisone
Doxorubicin (Adriamycin) or daunorubicin or a similar drug anthracycline
Based on the patient's prognosis, some schemes may also include cyclophosphamide (Cytoxan), L-asparaginase, etoposide (VP-16) and / or high-dose methotrexate or cytarabine (ara-C) as part of Induction .
For patients with ALL whose leukemia cells have a Philadelphia chromosome, a drug frequently also addressed as imatinib (Gleevec) is included.
The first month of treatment is quite intensive and requires frequent doctor visits. You can spend some or much of their time in the hospital because it may lead to serious infections or other complications. It is very important that your child take all the medicines prescribed. Some complications can be severe enough to endanger life. However, thanks to advances in supportive care (nursing care, nutrition, antibiotics, growth factors, transfusions of red blood cells and platelets as necessary, etc.) in recent years, these complications are much less common than in the past.
Most times the leukemia is in remission induction chemotherapy. However, because the leukemia cells can still be hidden somewhere in the body, it requires additional treatment.
Prophylaxis or treatment of central nervous system treatment to prevent leukemic cells from spreading to the central nervous system (prophylaxis) is similar to that used to treat leukemia that has spread to the CNS. This often begins during induction and continues through other stages of treatment. This may include one or more of the following:
Chemotherapy injected directly into the cerebrospinal fluid (intrathecal chemotherapy). The drug used most often is methotrexate, but sometimes you can also use cytarabine or a steroid such as prednisone. Intrathecal chemotherapy may be given during lumbar puncture (spinal) or through an Ommaya reservoir (this is discussed in the section on surgery).
High-dose methotrexate or cytarabine IV.
Radiation to the brain and spinal cord.
Consolidation (intensification)
If the leukemia is in remission, the next phase is often quite another short course chemotherapy, using many of the same drugs that were used in induction therapy. This usually takes several months. Usually the drugs are given in high doses, so the treatment is quite intense. During maintenance treatment, you can continue CNS prophylaxis. It also continues with a targeted drug such as imatinib, patients whose leukemia cells have the Philadelphia chromosome.
Some patients who are in remission, such as those with certain subtypes of ALL or other unfavorable prognostic factors are still at high risk of recurrence (return of leukemia). Doctors may suggest at this time an allogeneic stem cell transplantation (SCT), especially for those who have a brother or sister could be a good donor supported. An autologous stem cell transplant may be another option. It is necessary that the risks and potential benefits of stem cells for each patient according to their particular case carefully evaluated, because it is not yet clear how useful it is for each patient. Patients considering this procedure can get better service if you are in a center that has made many stem cell transplants, and should ask about do it as part of a clinical trial.
Maintenance
After consolidation, the patient is usually put on a maintenance program with chemotherapy consisting of methotrexate and 6-mercaptopurine (6-MP). In some cases this can be combined with other medications such as vincristine and prednisone.
For patients with ALL whose leukemia cells have the Philadelphia chromosome, frequently also addressed as medication imatinib is included.
Maintenance usually takes about two years. During maintenance treatment, you can continue CNS prophylaxis.
Some doctors feel that maintenance therapy may not be needed for some leukemias such as ALL of T cells and mature B-ALL (Burkitt leukemia) cells.
For patients with ALL whose leukemia cells have the Philadelphia chromosome, frequently also addressed as medication imatinib is included.
Maintenance usually takes about two years. During maintenance treatment, you can continue CNS prophylaxis.
Some doctors feel that maintenance therapy may not be needed for some leukemias such as ALL of T cells and mature B-ALL (Burkitt leukemia) cells.

Personal opinion: today I want to talk hacerca one of the treatments more comuñones to treat leukemia, which is chemotherapy, as it is a very vast subject, you speak out to them in stages, and I hope this information is to your liking and is clear and presisa that aya a good understanding.
bibliography
Gloria Rosen . (12/15/14). tratamiento leucemia . 26/10/2015, de american cancer society Sitio web: http://www.cancer.org/espanol/cancer/leucemialinfociticaagudaadultos/guiadetallada/leucemia-linfocitica-aguda-adultos-treating-typical-treatment
Wednesday 28 October 2015
Types of chemotherapy drugs

Chemotherapy drugs can be divided into several groups based on factors such as their mechanism of action, its chemical structure and its relationship with other medicines. Some drugs act in more than one way, and may belong to more than one group.
It is important to know the mechanism of action of a drug to predict side effects. This helps doctors decide which drugs may work well in combination. If you are using more than one drug, this information also helps them plan exactly when each drug should be given (the order and frequency).
Alkylating agents
Alkylating agents directly damage DNA (genetic material of each cell) to prevent the cell from reproducing. These drugs work in all phases of the cell cycle and are used to treat many different kinds of cancers, including leukemia, lymphoma, Hodgkin's disease, multiple myeloma and sarcoma, as well as cancers of the lung, Breast and ovarian cancer.
As these drugs damage DNA, they can cause long term damage to the bone marrow. In a few cases this can cause acute leukemia. Leukemia risk due to alkylating agents is dose dependent, which means that the risk is lower with lower doses, but increases as the total amount of drug used is increased. The risk of leukemia after administration of alkylating agents is the major approximately five to 10 years after treatment.
The alkylating agents are divided into different classes, including:
Nitrogen mustards: as mechlorethamine (nitrogen mustard), chlorambucil, cyclophosphamide (Cytoxan), ifosfamide and melphalan
Nitrosoureas: as streptozocin, carmustine (BCNU) and lomustine
Alkyl sulfonates: busulfan
Triazines: dacarbazine (DTIC) and temozolomide (Temodar®)
Ethylenimines: thiotepa and altretamine (hexamethylmelamine)
Platinum drugs (such as cisplatin, carboplatin and oxaliplatin) are sometimes grouped with alkylating agents because they kill cells similarly. These drugs are less likely to cause leukemia in the future that alkylating agents.
Antimetabolites
Antimetabolites interfere with the growth of DNA and RNA by substituting the key elements of these molecules. These agents damage cells during S phase, when cell chromosomes are copied. They are commonly used to treat leukemias, breast, ovary and the gastrointestinal tract as well as other cancers.
Examples of antimetabolites include:
5-fluorouracil (5-FU)
6-mercaptopurine (6-MP)
Capecitabine (Xeloda)
Cytarabine (Ara-C ®)
Floxuridine
Fludarabine
Gemcitabine (Gemzar)
Hydroxyurea
Methotrexate
Pemetrexed (Alimta)
Antitumor antibiotics
These drugs are not like antibiotics used to treat infections. Exert their action by altering the DNA in cancer cells to stop growing and multiplying.
Anthracyclines
Anthracyclines are antibiotic anticancer interfere with enzymes involved in DNA replication. These drugs work in all phases of the cell cycle and are widely used to treat various types of cancer.
Examples of anthracyclines include:
Daunorubicin
Doxorubicin (Adriamycin)
Epirubicin
Idarubicin
A major concern to be taken into account in the administration of these drugs is that they can permanently damage the heart if given in high doses. Therefore limits are frequently at doses of these drugs for life.
Other antibiotics against cancer
Anticancer antibiotics are not anthracyclines include:
Actinomycin D
Bleomycin
Mitomycin C Mitoxantrone (also acts as an inhibitor of topoisomerase II)
Topoisomerase inhibitors
These drugs interfere with topoisomerase calls that help separate the strands of DNA to be copied during S phase (Enzymes are proteins that cause chemical reactions in living cells) enzymes. Topoisomerase inhibitors are used to treat certain leukemias, as well as lung, ovarian, gastrointestinal and other.
Topoisomerase inhibitors are grouped according to the type of enzyme that affect.
Inhibitors of topoisomerase I include:
Topotecan
Irinotecan (CPT-11)
Inhibitors of topoisomerase II include:
Etoposide (VP-16)
Teniposide
Mitoxantrone (also acts as an anticancer antibiotic)
The topoisomerase II inhibitors may increase the risk of a second cancer (acute myeloid leukemia), as early as 2-3 years after medicine is given.
personal opinion, today I want to talk about the CHEMOTHERAPY treatment, this is the first part because the issue is very extensive, and this would be the first part of the treatment, I hope you enjoy it information.
bibliography
Gloria Rosen . (12/15/14). tratamiento leucemia . 28/10/2015, de american cancer society Sitio web: http://www.cancer.org/espanol/cancer/leucemialinfociticaagudaadultos/guiadetallada/leucemia-linfocitica-aguda-adultos-treating-typical-treatment
Friday October 30, 2015
How is chemotherapy administered?

Through a vein
Most chemotherapy drugs are administered directly into the bloodstream through a plastic tube called very small, flexible catheter. A needle is used to place a catheter into a vein in your hand or forearm; then the needle is removed while the catheter is placed. This is called intravenous or IV treatment. Intravenous drug can be administered in these ways:
The drugs can be rapidly administered through a catheter directly from a syringe in a few minutes, what is known as intravenous bolus.
Intravenous infusion can last from 30 minutes to several hours. A mixture of drugs flows from a plastic bag through the tube attached to the catheter. Often, the flow is controlled by a machine called intravenous pump.
Sometimes it is necessary to perform continuous infusions usually last from one to seven days. These are always controlled by electronic intravenous pumps.
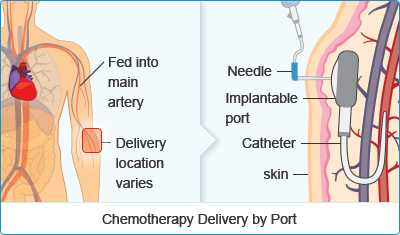
Needles and catheters can cause scarring or damage to the veins as chemotherapy is administered. Another option is the central venous catheter (CVC). The CVC is a larger catheter placed into a large vein in the chest or forearm. It remains in place for as long as the treatment, so that the insertion of a needle for each session is required to extend. A CVC, IV drugs may be administered more easily. One can also draw blood through the CVCs.
There are many different kinds of CVCs. Some consist of hoses inserted and exit through the skin, which makes use of syringes is not required. Another type is a port, which is a small cylinder with a thin tube inserted into the vein. Ports are permanently placed underneath the skin of the chest or arm during surgery. Then, to be used, special syringes are inserted through the skin into the port.
Many people talk to their doctor about the options CVCs even before starting treatment. Some find that during treatment need a CVC because the veins in your hands and arms are not in proper conditions to complete the planned chemotherapy treatment enough. Your doctor can help you decide if you need a CVC and CVC type suitable for you.
Alternatives
Depending on the drug and where the tumor is found, chemotherapy may also be administered in one or more of these ways:
Orally: this means that the drug is administered through the mouth. You swallow the chemotherapy drug in tablet, pill, tablet, capsule or liquid form like any other medicine. Generally, this method is more convenient because often chemotherapy can be administered at home. If you take oral chemotherapy drugs, it is very important that you take the right amount indicated in the schedule during the corresponding period. For more information, please read the document (available in English) Oral Chemotherapy: What You Need to Know.
Intrathecal: the drug is injected into the spinal canal to reach the fluid surrounding the brain and spinal cord. This fluid is called cerebrospinal fluid (CSF stands for). Chemotherapy entering the cerebrospinal fluid is transported to the brain and spinal cord. It may be fitted with a needle directly into his spine to quickly administer the drug or a catheter and port for long-term use is placed under the skin of his head during surgery. To this port is called Ommaya reservoir, which consists of a small device attached cylindrical shape having a small tube. The tube goes into the cerebrospinal fluid in the brain cavity and the port is placed under the scalp to the end of the treatment.
Intraarterially: the chemotherapy drug is delivered directly into an artery to treat one part of the body (such as liver, arm or leg). This method helps to limit the effect the drug has on other parts of the body, so it is called regional chemotherapy.
By intracavitary: chemotherapy drugs can be administered through a catheter into the abdominal cavity (the space around the intestines and other organs in the abdomen is known as intraperitoneal chemotherapy) or thoracic cavity (the space around lungs and other organs in the chest).
Intramuscularly: the medicine is given into a muscle through a needle (like a shot).
Intralesionally: a needle is used to administer the medication directly into a tumor in the skin, under the skin or into an internal organ.
Topically: medicine is placed directly on a region of skin cancer via a cream, jelly or ointment.
personal opinion, today I talk about another part of the quimioretapia, as given because roads this medicine is passed specific, the way in which it manages can be via intravesosa or oral, etc, it is very iportante know esacta amount of the drug for chemotherapy a success
bibliography
Gloria Rosen . (12/15/14). tratamiento leucemia . 30/10/2015, de american cancer society Sitio web: http://www.cancer.org/espanol/cancer/leucemialinfociticaagudaadultos/guiadetallada/leucemia-linfocitica-aguda-adultos-treating-typical-treatment
Monday, November 2 2015
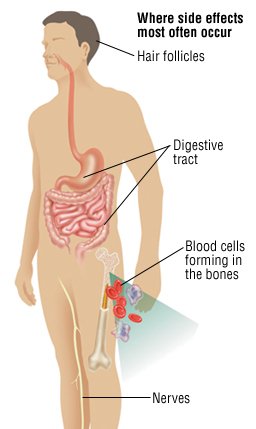
Side Effects During Treatment

The most significant disadvantage of chemotherapy is the development of treatment-related side effects. During treatment, you may experience a variety of gastrointestinal, musculoskeletal or constitutional symptoms. According to the National Cancer Institute (NCI), individuals undergoing chemo frequently report experiencing such symptoms as nausea, vomiting, loss of appetite, constipation or diarrhea. Fever and fatigue are also common side effects experienced by chemotherapy patients. The most apparent and emotionally challenging side effect associated with chemo treatment is alopecia--a medical condition in which your hair falls out. This condition may only affect certain areas of your body, such as the scalp, but may also extend to the face or limbs. The Mayo Clinic notes that chemo patients may also develop painful mouth sores or may bruise easily. Though these side effects may be significant, the majority of these symptoms will disappear once chemo treatment is stopped.

personal opinion :
today to conclude the issue I share chemotherapy, the side effects of this tramiento, as is chemotherapy as there are physiological changes in the body, and it is very important that they have in mind to not desconoscan that will occur after
BIBLIOGRAPHY
Gethy M . (Jun 25, 2015 ). disadvantages-chemotherapy. 2/11/2015, de livestrong Sitio web: http://www.livestrong.com/article/71774-disadvantages-chemotherapy/
Wednesday November 4, 2015
Drugs used in chemotherapy
Standard chemotherapy regimens include:

- AT: Adriamycin and Taxotere
- AC ± T: Adriamycin and Cytoxan, with or without Taxol or Taxotere
- CMF: Cytoxan, methotrexate, and fluorouracil
- CEF: Cytoxan, Ellence, and fluorouracil
- FAC: fluorouracil, Adriamycin, and Cytoxan
- CAF: Cytoxan, Adriamycin, and fluorouracil(The FAC and CAF regimens use the same medicines but use different doses and frequencies)
- TAC: Taxotere, Adriamycin, and Cytoxan
- GET: Gemzar, Ellence, and Taxol

Depending on the characteristics of the cancer, a targeted therapy medicine, such as Herceptin (chemical name: trastuzumab), may be used in combination with some chemotherapy regimens. For example, the TCH regimen includes Taxotere, Herceptin, and carboplatin.
Your doctor may talk about certain groups of chemotherapy medicines:
- Anthracyclines are chemically similar to an antibiotic. Anthracyclines damage the genetic material of cancer cells, which makes the cells die. Adriamycin, Ellence, and daunorubicin are anthracyclines.
- Taxanes interfere with the way cancer cells divide. Taxol, Taxotere, and Abraxane are taxanes.
Most standard chemotherapy regimens include a medicine from one or both of these groups.
PERSONAL OPINION: The purpose today is to introduce the name of the drugs most used in the administration of chemotherapy, which, as we had seen in the previous trattamiento Seciones is the most used in leukemia, then tell you about the mechanism of action of drugs that I mention today
bibliography
Michel. R . (October 20, 2015 at 11:53 AM). Chemotherapy Medicines. 4/11/15, de breascancer Sitio web: http://www.breastcancer.org/treatment/chemotherapy/medicines
Friday November 6, 2015
Can I work while receiving chemotherapy?

Fatigue due to chemotherapy
Side effects of chemotherapy
What causes side effects?
Cancer cells grow rapidly, and the chemo drugs kill rapidly growing cells. However, because these drugs circulate throughout the body, they can affect normal, healthy cells grow too quickly. The cause of the side effects is the damage to healthy cells. Side effects are not always as bad as you might expect, but many people are concerned about this part of cancer treatment.
The normal cells most likely to be damaged by chemotherapy are the blood-forming cells in the bone marrow and cells in the mouth, digestive tract, reproductive system and hair follicles. Some chemotherapy drugs can damage cells of the heart, kidneys, bladder, lungs and nervous system. In some situations, you can administer chemotherapy drugs to help protect normal cells of the body.
What should I know about side effects?
Not everyone will experience all of the side effects, some people experience few, if they get to experience something.
The severity of side effects (how bad are) varies greatly according to the person. Be sure to talk to your doctor or nurse about the most common side effects of chemotherapy, how long will last, how serious can be and when to call the doctor's office. For more information, see "When can consult the doctor about side effects of chemotherapy?".
It is possible that your doctor gives you medicine that will help prevent some side effects before they occur.
Some types of chemotherapy cause long-term side effects such as heart conditions or damage to nerves as well as fertility problems. However, many people have no term problems caused by chemotherapy. Consult your doctor about the risks of long-term chemotherapy drugs you are getting.
While side effects may cause discomfort, they must be balanced against the need to destroy cancer cells.
How long are the side effects?
Most side effects slowly go away after treatment ends because the healthy cells recover with the passage of time. The time it takes to overcome the side effects and regain strength varies in each person. It depends on many factors, including your overall health and drugs you are given.
Many side effects go away fairly quickly, although some take months or even years to disappear completely. Sometimes the side effects can last a lifetime; Such is the case when chemotherapy causes long-term damage to the heart, lungs, kidneys or reproductive organs. Certain types of chemotherapy sometimes cause delayed effects, such as a second cancer, that show up many years later.
Often people are put off by the duration of treatment or suffer side effects. If you feel this way, talk to your doctor. It may be that you can make a change in medication or treatment program. Perhaps your doctor or nurse also have suggestions about ways to reduce any pain or discomfort.

What are the common side effects?
Most people worry about whether or not to have side effects due to chemotherapy, and if so, how will that effect. The following is a summary of some of the most common side effects caused by chemotherapy. We also share some tips on how to control them.
Personal opinion. to conclude the issues of chemotherapy, it is important to mention that this my treatment side effects are risks where the patient suffering them under the effects of chemotherapy drugs
Blibliography
Gloria Rosen . (08/10/2015). guia sobre quimioterapia . 6-nov-2015, de carncer Sitio web: http://www.cancer.org/espanol/servicios/tratamientosyefectossecundarios/quimioterapia/fragmentado/quimioterapia-una-guia-para-los-pacientes-y-sus-familias-chemo-side-effects
Monday November 8, 2015
Nutrition for people with leukemia
Leukemia is a disease that is caused by an overproduction of white blood cells (leukocytes), which are the cells that make blood and tissue involved in defending the body against foreign substances or infectious agents (antigens).
For this condition, it is recommended to follow a proper diet, which is one of the fundamental bases to treat and even cure this condition.
Routine food must be of high quality, removing toxic and harmful foods like white flour or refined, white sugar and derivatives, as well as sausages, fried pickles, vinegar, processed, fried, red meat, etc. In the diet should include plenty of fresh vegetables and fruits and seeds.

For adults, it is recommended to undergo a preliminary cleansing diet, for three consecutive days eating a single fruit like grapes, papaya, oranges, etc. and two liters of pure water. Then, start with diet proposal, including some little food to the diet.
Recommended foods and supplements: soy and its derivatives are a great option for people with leukemia. In addition, to include vegetable broths, fresh juices and varied with different vegetables a day and food consumption rivers in vitamin C such as oranges, lemons, onions, etc. Foods that are a must in the diet include garlic, onions, citrus fruits, brown rice, berries, seeds, tomato, broccoli, celery, soy, tofu, bean sprouts, alfalfa, amaranth, lentils, vegetable milks (replacing Cow's milk), tea and green tea (replacing all sugary drinks and processed).
Personal opinion: I wanted to talk today a fundamental issue for tratameinto leukemia, diet must be carried relation to the disease, it is very important to be balanced for an allocation beyond the loss of proteins, which are removed by treating chemotherapy, I hope this information is of degree sua
bibliographya :Laura Garces . (5/9/2013). Recetas y dieta para niños y personas con Leucemia. 8-11-15, de Biomanantial Sitio web: http://www.biomanantial.com/recetas-dieta-para-ni%C3%B1os-personas-con-leucemia-a-2218-es.html
Wednesday 11th November 2015
Changes in lifestyle after treatment of chronic myeloid leukemia
You can not change the fact that he had cancer. What we can change is how you live the rest of his life to make decisions that help you stay healthy and feel as well as you possibly can. It may be time to reassess various aspects of his life. Maybe he's thinking about how you can improve your health in the long term. Some people even start these changes during treatment.

Making healthier choices
For many people, a diagnosis of cancer helps them focus on their health in ways they may not have thought in the past. What things could you do to be a healthier person? Maybe you could try to eat more healthy foods or exercise more. Perhaps you could reduce the consumption of alcoholic beverages or leave the snuff. Even things like keeping your stress level under control may help. This is a good time to think about making changes that can have positive effects for the rest of his life. You'll feel better and also be healthier (a).
You can start by addressing the aspects that most anxious. Get help for those that are most difficult. For example, if you are thinking about quitting smoking and need help, call the American Cancer Society for information and support. This service support smoking cessation can help increase your chances of quitting the snuff forever.
Eating better
Eating right can be hard for anyone, but it can be even tougher during and after cancer treatment. Treatment may change your sense of taste. Nausea can be a problem. It may not feel like eating and lose weight unintentionally. Or maybe you can not remove the weight has gone up. All these things can be very frustrating.
If treatment caused weight changes or problems with feeding or taste, do the best you can and remember that these problems usually improve over time. You may find it helps to eat small portions every 2 to 3 hours until you feel better. You can also ask your cancer team about consulting with a nutritionist (a nutritionist) who can give you ideas about how to deal with these side effects of treatment.
One of the best things you can do after cancer treatment is to adopt healthy eating habits. Maybe you would be surprised the long-term benefits of some simple changes, like increasing the variety of healthy foods you eat. Achieving and maintaining a healthy weight, eating a healthy diet, and limiting your alcohol intake may lower your risk of developing several types of cancer. In addition, having many other health benefits. For more information, see our document called Nutrition and Physical Activity During and After Cancer Treatment Answers to Common Questions.
Personal opinion: today touch them the subject of performing activities to be treating people with leukemia is very important that beyond the support of family and people around them so that there is mtivacion
Gloria Rosen . (04/13/2015). cambios en estilo de vida a personas con leucemia . 11 -11-15, de América cancer Sitio web: http://www.cancer.org/espanol/cancer/leucemiamieloidemielogenacronica/guiadetallada/leucemia-mieloide-mielogena-cronica-after-lifestyle-changes
Friday November 13, 2015
Rest, fatigue and exercise
Extreme tiredness, called fatigue, is very common in people treated for cancer. This is not a normal type of tiredness but a tiredness that is not relieved by rest. For some people, fatigue lasts a long time after treatment, and may find it difficult to exercise and do other activities they wish to pursue. Studies have shown that patients who follow an exercise program tailored to their personal needs feel better physically and emotionally and can cope better with your situation.

If you were sick (a) and not very active (a) during treatment, it is normal to have lost some of its fitness, muscular strength and endurance. Any plan for physical activity should fit your own situation. A person who has never exercised will not make the same amount of exercise as a playing tennis twice a week. If you have not exercised in a few years, you will have to start slowly. Maybe just by taking short walks.
Talk to the team of the health care team before starting. Ask them what they think about your exercise plan. Then, try to get someone to accompany you to exercise so that not doing it alone. The company of family or friends to start a new exercise program can give you that extra stimulus to keep it going when the will is not enough.
If you are very tired, you will need to balance activity with rest. Occasionally, some people find it really difficult to take breaks when they are used to working all day or taking care of the home. However, this is not the time to be very demanding with yourself. Be aware of what your body and rest when needed. For more information on coping with fatigue, please see our document, Fatigue in People With Cancer and Anemia in People With Cancer.
Note that exercise can improve your physical and emotional health:
It improves your cardiovascular (heart and circulation)
Along with good nutrition, will help you achieve and maintain a healthy weight
It strengthens your muscles
It reduces fatigue and helps you have more energy
It helps to reduce anxiety and depression
It can make you feel happier
It helps you feel better about yourself
In addition, long-term, we know that getting regular physical activity plays a role in helping to reduce the risk of some cancers. Regular physical activity also provides other benefits to health.
Personal opinion: I speak today of a continuation of the activities undertaken to individuals pursuing a disease of leukemia, but today I focus more on the cansancion that exists in them as well as the rest you must have
bibliography
Gloria Rosen . (04/13/2015). cambios en estilo de vida a personas con leucemia . 13 -11-15, de América cancer Sitio web: http://www.cancer.org/espanol/cancer/leucemiamieloidemielogenacronica/guiadetallada/leucemia-mieloide-mielogena-cronica-after-lifestyle-changes
Monday, November 16
This section outlines treatments that are the standard of care (the best proven treatments available) for this specific type of cancer. To make decisions regarding the treatment plan, it is also strongly advises patients to consider the option of participating in clinical trials. A clinical trial is a research study to test a new approach to treatment in order to assess whether this is safe, effective, and possibly better than standard treatment. Clinical trials can test these approaches, as in the case of a new drug, a new combination of standard doses of existing or new therapies. Your doctor can help you review all treatment options. For more information, see the Clinical Studies sections and latest research.
Treatment overview
In cancer care, often they work together different types of doctors to create a comprehensive treatment plan that combines different types patient treatment. This is called a multidisciplinary team (in English).
Here are the most common treatment options for AML are described. Options and treatment recommendations depend on several factors, including the subtype, morphology and cytogenetics of AML (see Subtypes), possible side effects and patient preferences and your overall health. Your care plan may also include treatment for symptoms and side effects, an important part of cancer care.
The most successful treatment for AML depends on the results of the first treatment; therefore, it is important for patients undergoing their first treatment at a center with experience in AML.
Take time to learn about all treatment options and be sure to ask questions about things that are unclear. Also, talk to your doctor about the objectives of each treatment and what to expect while receiving treatment. Learn more about how to make decisions about the treatment,
Personal opinion: I'll give an introduction today of care in the treatments performed to control leukemia hope this will be useful information
Bibliography
Junta Editorial de Cancer.Net,. (11/2014). Leucemia - mieloide aguda - AML - en adultos: Opciones de tratamiento. 16/11/2015, de LEUCEMIA.COM Sitio web: http://www.cancer.net/es/tipos-de-c%C3%A1ncer/leucemia-mieloide-aguda-aml-en-adultos/opciones-de-tratamiento
Wednesday November 18, 2015
Intensive chemotherapy
Chemotherapy is the use of drugs to kill cancer cells, usually by inhibiting their ability to grow and divide. The drugs travel through the bloodstream to reach cancer cells throughout the body. A medical oncologist, who specializes in treating cancer with medication, or a hematologist, a doctor who specializes in treating blood disorders, doctor are those who administer chemotherapy.
Chemotherapy is the primary treatment for AML. Systemic chemotherapy is delivered through the bloodstream to reach cancer cells throughout the body. Some common methods of administering chemotherapy include intravenous (IV) tube that is placed into a vein with a needle injection into the cerebrospinal fluid, or a pill or capsule is swallowed (oral). Chemotherapy may also be given as an injection under the skin, which is called subcutaneous injection. If chemotherapy is administered intravenously, it can be applied on a larger vein or smaller; for example, in the arm. If administered in a large vein, it may need to place a central venous catheter or port in the body. A chemotherapy regimen or program usually consists of a specific number of treatments given over a period of time. A patient may receive a drug time or combinations of different drugs at the same time. Many drugs are used to treat AML, which are discussed below.
Learn more about chemotherapy and preparing for treatment. Medications used to treat cancer are continually being evaluated. Often, talk with your doctor is the best way to learn about the medications prescribed for you, their purpose and their potential side effects or interactions with other medicines. Learn more about your prescriptions by drug databases in which drugs can be searched
Personal opinion: I share today on this subject intejnsiva chemotherapy anteriornmente already mentioned, but it is important in different aspects profundise
Bibliography
Junta Editorial de Cancer.Net,. (11/2014). Leucemia - mieloide aguda - AML - en adultos: Opciones de tratamiento. 18/11/2015, de LEUCEMIA.COM Sitio web: http://www.cancer.net/es/tipos-de-c%C3%A1ncer/leucemia-mieloide-aguda-aml-en-adultos/opciones-de-tratamiento
Friday November 20, 2015
Child with acute non–lymphoblastic leukemia and hyperleukocytosis
clinic history
10-year-old from Coyuya, Guerrero, who went to a children's hospital of tertiary care with the following: presence of bilateral cervical lymph 20 days of evolution, sudden onset and progressive growth, without hyperemia or changes local temperature; while presented fatigue, weakness and pallor, initially on the face and then exacerbated widespread that a week earlier. Two weeks before admission, he presented dysphonia progressive admission that prevented him from speaking. Ten days before he began with colicky abdominal pain located in hypogastrium with bilateral irradiation hypochondria that was exacerbated by palpation; also he presented painless without predominance of schedule eyelid edema. Three days before it was added to the box dermatosis characterized by purplish macules of about 2.0 mm in diameter, face, chest and arms. Four days before admission was hospitalized in their place of origin; however, he went to the hospital by their own means and did not mention the clinical summary instituted treatment. Among its highlights peasant background father and smoking. The other inherited family history, personal pathological perinatal and irrelevant to the current condition.
Physical examination: weight 35.5 kg (p50), height 132 cm (PLO), heart rate 112 per minute, respiratory rate 18 per minute, blood pressure 110/70 mm Hg, afebrile, alert, responsive, had generalized pallor, petechiae 1.0 to 2.0 mm in diameter on the face, chest, arms and abdomen, ears unaltered, gingival hyperplasia and hypertrophy of palatine tonsils level III. Bilateral neck volume increased at the expense of mobile nodes, painless, discoloration or temperature. Supraclavicular nodes of 0.5 cm in diameter, hard and painful on palpation were also found. The chest auscultation, systolic murmur grade II left second intercostal space, well-ventilated lung fields; abdominal soft, without tenderness, liver edge 8, 7 and 7 cm below the costal margin, spleen to 5, 5 and 6 cm below the costal margin. Bilateral inguinal lymphadenopathy of unspecified size. Neurological examination was normal. The rest of the physical examination, no relevant data. Laboratory studies were requested and bone marrow aspirate

Personal opinion: the most important of nursing care is to perform an adequate physical examination, likewise we determine what the patient needs and prioritize needs on a timely care, dcompartir wanted them today as it is a medical history where a specific assessment is made and the patient's needs are described
bibliography
Glenda Juárez–Caballero. (02-2007). Child with acute non–lymphoblastic leukemia and hyperleukocytosis.. 20-11-15, de scielo Sitio web: http://www.scielo.org.mx/scielo.php?pid=S1665-11462007000100009&script=sci_arttext
Monday November 23, 2015
Nursing interventions for children with leukemia
Nursing Care Plans
The care plan for patients with leukemia should be emphasized on comfort, minimize the adverse effects of chemotherapy, promote preservation of veins, manage complications, and provide teaching and psychological support. Here are 5 leukemia nursing care plans (NCP).
1. Risk for Infection

Risk factors may include
- Inadequate secondary defenses: alterations in mature WBCs (low granulocyte and abnormal lymphocyte count), increased number of immature lymphocytes; immunosuppression, bone marrow suppression (effects of therapy/transplant)
- Inadequate primary defenses (stasis of body fluids, traumatized tissue)
- Invasive procedures
- Malnutrition; chronic disease
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Identify actions to prevent/reduce risk of infection.
- Demonstrate techniques, lifestyle changes to promote safe environment, achieve timely healing.
Personal opinion: I wanted to talk to them today about an introduction of nursing interventions where are reflected plamados care and knowledge of the nurse, who graacias to that patients presenting with these diseases lead a quieter life by tratamintos and nurses available drugs that manage them
bibligraphy
M. Walter. (27-feb2014). leukeimia nursing . 23/nov-2015, de medical nursing Sitio web: http://nurseslabs.com/5-leukemia-nursing-care-plans/
| Nursing Interventions | Rationale |
|---|---|
| Place in a private room. Limit visitors as indicated. Prohibit live plants or flowers. Restrict fresh fruits and make sure they are properly washed or peeled. Coordinate patient care so that leukemic patient doesn’t come in contact with staff who also care for patients with infections or infectious diseases. | To protect the patient from potential sources of pathogens or infection. Bone marrow suppression, neutropenia, and chemotherapy places the patient at high risk for infection. |
| Require good hand washing protocol for all personnel and visitors. | Prevents cross-contamination and reduces risk of infection. |
| Closely monitor temperature. Note correlation between temperature elevations and chemotherapy treatments. Observe for fever associated with tachycardia, hypotension, subtle mental changes. | Although fever may accompany some forms of chemotherapy, progressive hyperthermia occurs in some types of infections, and fever (unrelated to drugs or blood products) occurs in most leukemia patients. Septicemia may occur without fever. |
| Prevent chilling. Force fluids, administer tepid sponge bath. | Helps reduce fever, which contributes to fluid imbalance, discomfort, and CNS complications. |
| Encourage frequent turning and deep breathing. | Prevents stasis of respiratory secretions, reducing risk of atelectasis or pneumonia. |
| Auscultate breath sounds, noting crackles, rhonchi. Inspect secretions for changes in characteristics: increased sputum production or change in sputum color. Observe urine for signs of infection: cloudy, foul-smelling, or presence of urgency or burning with voids. | Early intervention is essential to prevent sepsis in immuno-suppressed person. |
| Handle patient gently. Keep linens dry and wrinkle-free. | Prevents sheet burn and skin excoriation. |
| Inspect skin for tender, erythematous areas; open wounds. Cleanse skin with antibacterial solutions. | May indicate local infection. Open wounds may not produce pus because of insufficient number of granulocytes. |
| Inspect oral mucous membranes. Provide good oral hygiene. Use a soft toothbrush, sponge, or swabs for frequent mouth care. | The oral cavity is an excellent medium for growth of organisms and is susceptible to ulceration and bleeding. |
| Avoid using indwelling urinary catheters and giving I.M. injections. | These can provide an avenue for infection. |
| Provide thorough skin care by keeping the patient’s skin and perianal area clean, apply mild lotion or creams to keep the skin from drying or cracking. Thoroughly clean skin before all invasive skin procedures. | Additional measures to avoid infection. |
| Change IV tubing according to your facility’s policy. Use strict sterile technique and a metal scalp vein needles (metal butterfly needle) when starting IV. If the patient receives total parenteral nutrition, give scrupulous subclavian catheter care. | IV sites can harbor infection. Additional measure to avoid infection. |
| Promote good perianal hygiene. Examine perianal area at least daily during acute illness. Provide sitz baths, using Betadine or Hibiclens if indicated. Avoid rectal temperatures, use of suppositories. | Promotes cleanliness, reducing risk of perianal abscess; enhances circulation and healing. Perianal abscess can contribute to septicemia and death in immune compromised patients. |
| Coordinate procedures and tests to allow for uninterrupted rest periods. | Conserves energy for healing, cellular regeneration. |
| Encourage increased intake of foods high in protein and fluids with adequate fiber. | Promotes healing and prevents dehydration. Constipation potentiates retention of toxins and risk of rectal irritation or tissue injury. |
| Limit invasive procedures (venipuncture and injections) as possible. | Break in skin could provide an entry for pathogenic or potentially lethal organisms. Use of central venous lines (tunneled catheter or implanted port) can effectively reduce need for frequent invasive procedures and risk of infection. Myelo suppression may be cumulative in nature, especially when multiple drug therapy (including steroids) is prescribed. |
| Monitor laboratory studies: | |
| CBC, noting whether WBC count falls or sudden changes occur in neutrophils; | Decreased numbers of normal or mature WBCs can result from the disease process or chemotherapy, compromising the immune response and increasing risk of infection. |
| Gram’s stain cultures and sensitivity. | Verifies presence of infections; identifies specific organisms and appropriate therapy. |
| Review serial chest x-rays. | Indicator of development or resolution of respiratory complications. |
| Prepare for and assist with leukemia-specific treatments such as chemotherapy, radiation, and/or bone marrow transplant. | Leukemia is usually treated with a combination of these agents, each requiring specific safety precautions for patient and care providers. |
| Administer medications as indicated: | |
| antibiotics | May be given prophylactically or to treat specific infection. |
| Colony-stimulating factors: sargramostim (Leukine). | Restores WBCs destroyed by chemotherapy and reduces risk of severe infection and death in certain types of leukemia. |
| Avoid use of aspirin-containing antipyretics. | Aspirin can cause gastric bleeding and further decrease platelet count. |
| Provide nutritious diet, high in protein and calories, avoiding raw fruits, vegetables, or uncooked meats. | Proper nutrition enhances immune system. Minimizes potential sources of bacterial contamination. |
personal opinion: Throughout the weeks speak to them of leukemia complications and others, in this section I focus unicamnete to care and activities of the professional enfemereia for coping patient, thank you nursing works with values, honesty , to keep integral care of the patient should be treated and cared for in the best m, w ay possible
bibligraphy
M. Walter. (27-feb2014). leukeimia nursing . 25/nov-2015, de medical nursing Sitio web: http://nurseslabs.com/5-leukemia-nursing-care-plans/
Friday November 27, 2015
Clinical case
Male patient, 17, no morbid history of relevance, that two months before admission started upper respiratory condition characterized by hoarseness, sore throat, nasal congestion, chills and night unquantified feverish feeling. He received different antibiotics on an outpatient treatments without clinical improvement. Computed tomography (CT) showed sinus pansinusitis and nasofibroscopy who reported "scabby laryngitis", indicating antibiotics and oral and inhaled corticosteroids was performed.
It evolved with febrile temperature of 39 ° C and laryngeal stridor, why he consulted to the emergency department where his hospitalization is decided.
He was evaluated by an otolaryngologist, performing endoscopy, which showed a crusty lesion with decreased glottic laryngeal lumen caliber. The income CBC showed 40% hematocrit, Hb 13.5, leukocytes 4,700
RAN 2700, normal platelets, sedimentation rate of 20 mm.
antibiotics, steroids and nebulized respiratory symptoms improvement and remission of fever began. Seven days after new endoscopic examination, which showed decrease of crusted lesions with new lesions granulomatous appearance was made. Given these findings, it was decided to perform biopsy and making crops flag under direct laryngoscopy. During surgery, the patient developed fever and profuse bleeding. Tests showed pavilion taken Hct of 37%, 74,000 leukocytes and platelets 900.
He was taken to the surgical ICU where he quickly developed respiratory failure requiring mechanical ventilation.
At that time, given the emergence of pancytopenia, was evaluated by hematology, bone marrow biopsy effected, Myelogram sucked and flow cytometry.
Within 48 hours, the patient developed rapidly progressive multiple organ failure with respiratory compromise, renal and coagulopathy associated with refractory shock to vasoactive drugs and antibiotic and antifungal spectrum coverage, requiring ventilatory support, dialysis and blood products
Clinical case
Male patient, 17, no morbid history of relevance, that two months before admission started upper respiratory condition characterized by hoarseness, sore throat, nasal congestion, chills and night unquantified feverish feeling. He received different antibiotics on an outpatient treatments without clinical improvement. Computed tomography (CT) showed sinus pansinusitis and nasofibroscopy who reported "scabby laryngitis", indicating antibiotics and oral and inhaled corticosteroids was performed.
It evolved with febrile temperature of 39 ° C and laryngeal stridor, why he consulted to the emergency department where his hospitalization is decided.
He was evaluated by an otolaryngologist, performing endoscopy, which showed a crusty lesion with decreased glottic laryngeal lumen caliber. The income CBC showed 40% hematocrit, Hb 13.5, leukocytes 4,700
RAN 2700, normal platelets, sedimentation rate of 20 mm.
antibiotics, steroids and nebulized respiratory symptoms improvement and remission of fever began. Seven days after new endoscopic examination, which showed decrease of crusted lesions with new lesions granulomatous appearance was made. Given these findings, it was decided to perform biopsy and making crops flag under direct laryngoscopy. During surgery, the patient developed fever and profuse bleeding. Tests showed pavilion taken Hct of 37%, 74,000 leukocytes and platelets 900.
He was taken to the surgical ICU where he quickly developed respiratory failure requiring mechanical ventilation.
At that time, given the emergence of pancytopenia, was evaluated by hematology, bone marrow biopsy effected, Myelogram sucked and flow cytometry.
Within 48 hours, the patient developed rapidly progressive multiple organ failure with respiratory compromise, renal and coagulopathy associated with refractory shock to vasoactive drugs and antibiotic and antifungal spectrum coverage, requiring ventilatory support, dialysis and blood products
Clinical case
Male patient, 17, no morbid history of relevance, that two months before admission started upper respiratory condition characterized by hoarseness, sore throat, nasal congestion, chills and night unquantified feverish feeling. He received different antibiotics on an outpatient treatments without clinical improvement. Computed tomography (CT) showed sinus pansinusitis and nasofibroscopy who reported "scabby laryngitis", indicating antibiotics and oral and inhaled corticosteroids was performed.
It evolved with febrile temperature of 39 ° C and laryngeal stridor, why he consulted to the emergency department where his hospitalization is decided.
He was evaluated by an otolaryngologist, performing endoscopy, which showed a crusty lesion with decreased glottic laryngeal lumen caliber. The income CBC showed 40% hematocrit, Hb 13.5, leukocytes 4,700
RAN 2700, normal platelets, sedimentation rate of 20 mm.
antibiotics, steroids and nebulized respiratory symptoms improvement and remission of fever began. Seven days after new endoscopic examination, which showed decrease of crusted lesions with new lesions granulomatous appearance was made. Given these findings, it was decided to perform biopsy and making crops flag under direct laryngoscopy. During surgery, the patient developed fever and profuse bleeding. Tests showed pavilion taken Hct of 37%, 74,000 leukocytes and platelets 900.
He was taken to the surgical ICU where he quickly developed respiratory failure requiring mechanical ventilation.
At that time, given the emergence of pancytopenia, was evaluated by hematology, bone marrow biopsy effected, Myelogram sucked and flow cytometry.
Within 48 hours, the patient developed rapidly progressive multiple organ failure with respiratory compromise, renal and coagulopathy associated with refractory shock to vasoactive drugs and antibiotic and antifungal spectrum coverage, requiring ventilatory support, dialysis and blood products
Personal opinion: today I want to talk about a case of a type of leukemia that podemosmencontrar, on this occasion the situation of pacviente described as the disease progresses
Bibliography : Dr. Mario Guerrero. (Abril 2005). caso clinico . 27-11-15, de revista medica chilena Sitio web: http://www.scielo.cl/scielo.php?pid=S0034-98872005000400010&script=sci_arttext
Clinical case
Dona Maria is a woman of 72 years old, which is followed in February 2012 by the Primary Care Team (EAP) in their area of health, symptom control and observation of their neoplastic disease. Since his discharge in February 2012, the primary care team went to valuation and control once a week, until, at 2 months, Mary noticed an increase in pain and analgesia scheduled doses did not feel relief. Mary calls her nurse reference in the EAP because it can not tolerate this situation, and needs to improve his current state of health, it relieves your present suffering. It was reported that the EAP process, who went to new multidisciplinary assessment and review of the treatment planned.
With the next job is to describe the case of a patient of our team, through the model of Dorothea Orem, evaluating, diagnosing, planning, implementing and evaluating care to follow, using the NANDA, NOC and NIC taxonomy without forgetting that process is circular. We will focus mainly on the management and pain control, to stress the importance that represents this data as a value in a vital fifth constant, since the deterioration of health by the patient tells us is pain suffering because of their neoplastic process.
Personal opinion, today I am placing a clinical case, it is therefore important that we enfeermeras comno control as pacinete that this comes with advanced disease
Bibliography: Miriam Paula Marcos Espino . (Dic 2013). Aplicación del modelo de Dorothea Orem ante un caso de una persona con dolor neoplásico. 30-11-15, de scielo Sitio web:
Wednesday December 2, 2015
Nursing diagnosis.- Risk of infection r / c leucopenia, malnutrition, immunosuppression and gateway.- Nutritional imbalance default r / c vomiting, taste disturbances, stomatitis, ulcers, nausea, anorexia m / p weight loss, body mass loss, weakness, fatigue and malaise.- Intolerance to physical activity r / c dyspnea, fatigue, bone pain and decreased erythrocyte m / p tachycardia, dyspnea, tachypnea, has this to any difficulty.- Risk of injury r / c bleeding and infiltration of the CNS, spleen, liver and cystitis.- Alteration of body image r / c alopecia, paleness, weight loss, moon facies and bruises m / w changes in mood, isolation, depression and crying.- Fear r / c possibility of a fatal outcome, bad prognosis, rapid evolution m / p irritability, crying, depression, verbalization and changes in mood.- Impairment of oral mucosa or perianal r / c chemotherapy Myelosuppression m / p ulcerations, gingival, mucositis and stomatitis.- Early Mourning.- Constipation.- Pain.- Ineffective family coping.- Impaired physical mobility.- Risk or fluid volume deficit r / c hyperthermia, vomiting, diarrhea m / w dry skin, sunken eyes etc.Nursing objectives.Avoid injury.Avoid malnutrition.Emotional support.Prevent complications.General care.Prepare the family and the child to the diagnostic and treatment procedures.Ease the pain.Prevent complications of myelosuppression.Take precautions when handling and administering chemotherapeutic agents.Deal with problems due to drug toxicity.Provide physical care and emotional support.Specific care to prevent bleeding.Change position to promote circulation.Keep it stable.Away from any object that causes injury.Do not administer drugs with aspirin.Avoid unnecessary punctures or invasive techniques.Specific care to prevent infection.Avoid contact with infected persons.Promote isolation.Practice thorough washing hands.Monitor signs of infection such as elevated temperature, redness areas or areas of heat.Provide general health of the child.If you need to handle with sterile technique.Avoid vaccines.Provide adequate nutrition.Avoid unnecessary punctures.Specific care for fluid volume imbalance.Control and fluid balance.Encourage hydration.Increased intake.Assess the state of hydration.Specific care for pain.Providing massage.Distract the patient in different ways.Providing analgesic if necessary.Placing physical media.Keep the rest.Immobilize the member who is in pain.Promote the games.Specific care for constipation.Provide a high intake of water.Foods with fiber handle.Apply massage on the stomach.Specific care for the deterioration of the oral mucosa.Recommend the use of toothbrushes with soft bristles.Maintaining good hydration.Provide mouthwashes with bicarbonate water before eating.Eating soft foods, based on a bland diet.Specific care for the deterioration of the anal mucosa.Toilet increasingly evacuate the child with mild soap and water.Specific care for nutritional imbalance by default.Providing food in small portions more often.Oral hygiene.Watch vomiting.Weigh daily.Provide food which is the taste of the patient.Rate preferences in choosing food.Avoid extremes in flavors.Specific care for impaired physical mobility.Encourage periods of activity and rest.Specific care for lack of recreational activities.Promote the game, read books and paint or draw.Specific care of body image disorder.Encourage the use of wigs, hats or handkerchief.Explain to the child that the treatment of transient and reversible changes
personal opinión , today nurses develop a critical role in the care to pcnet therefore perform interventions according to the needs of each, I present one tablespoon planned activities as on requirements
bibliograhya : Lic. ENFE. REBECA. S. (domingo, 5 de julio de 2009). leucemia y sus cuidados . 2-12-2015, de enfermeria ciencias Sitio web: http://eenfermeriauv.blogspot.mx/2009/07/leucemia-panorama-general-y-cuidados-de.HTML
very good!!! :)
ResponderBorrarMost prostate cancers are adenocarcinomas, cancers that arise in glandular cells of the prostate’s epithelial tissue. Prostate cancers usually progress slowly and produce no symptoms in the initial stages. Eventually, the tumor may enlarge like mine too, the prostate gland, pressing on the urethra and causing painful or frequent urination and blood in the urine. So I was so uncomfortable with this prostate cancer diseases then I decided to do online search on how to cure cancer because I well have read a lot about herbal medicine, I came across a lot of testimony how Dr Itua cure HIV/herpes then Cancer was listed below the comment.with courage I contacted Dr Itua and he sent me his herbal medicine through Courier service then I was asked to pick it up at my post office which i quickly did. I contacted Dr Itua that I have received my herbal medicine so he instructed me on how to drink it for three weeks and that is how Dr Itua Herbal Medicine cures my prostate Cancer, The treatment takes three weeks and I was cured completely. Dr Itua is a god sent and I thank him every day of my life. Contact him now On: Email:drituaherbalcenter@gmail.com/ Whatsapp:+2348149277967. He listed that he can as well cure the following diseases below.... Cerebral Amides. Lung Cancer,Brain cancer,Esophageal cancer,Gallbladder cancer,Gestational trophoblastic disease,Head and neck cancer,Hodgkin lymphoma Intestinal cancer,Kidney cancer,Leukemia,Liver cancer,Melanoma,Mesothelioma,Multiple myeloma,Neuroendocrine tumors,Hodgkin lymphoma,Oral cancer,Ovarian cancer,Sinus cancer,Soft tissue sarcoma,Spinal cancer,Stomach cancer,Meniere's disease , Testicular cancer,Throat cancer,Thyroid Cancer,Uterine cancer,Vaginal cancer,Vulvar cancer. Alzheimer's disease,Autism,measles, tetanus, whooping cough, tuberculosis, polio and diphtheria Adrenocortical carcinoma. Alma, Uterine Cancer, Breast Cancer, Allergic diseases. Kidney cancer, Love Spell, Glaucoma., Cataracts,Macular degeneration,Cardiovascular disease,Lung disease.Enlarged prostate,Osteoporosis.Generalized dermatitis,Alzheimer's disease,Brain Tumor,Lupus,Endometrial Cancer, cerebrovascular diseases
ResponderBorrarDementia.Colo rectal cancer, Lottery Spell, Bladder Cancer, Skin Cancer,Ovarian Cancer,Pancreatic Cancer, HIV /Aids,Brain Tumor, Herpes, Non-Hodgkin lymphoma, Inflammatory bowel disease, Copd, Diabetes, Hepatitis